The Statement
A social media post claims the efficacy rates of four COVID-19 vaccines are far lower than those claimed by vaccine companies, citing figures from a "peer reviewed study" as evidence.
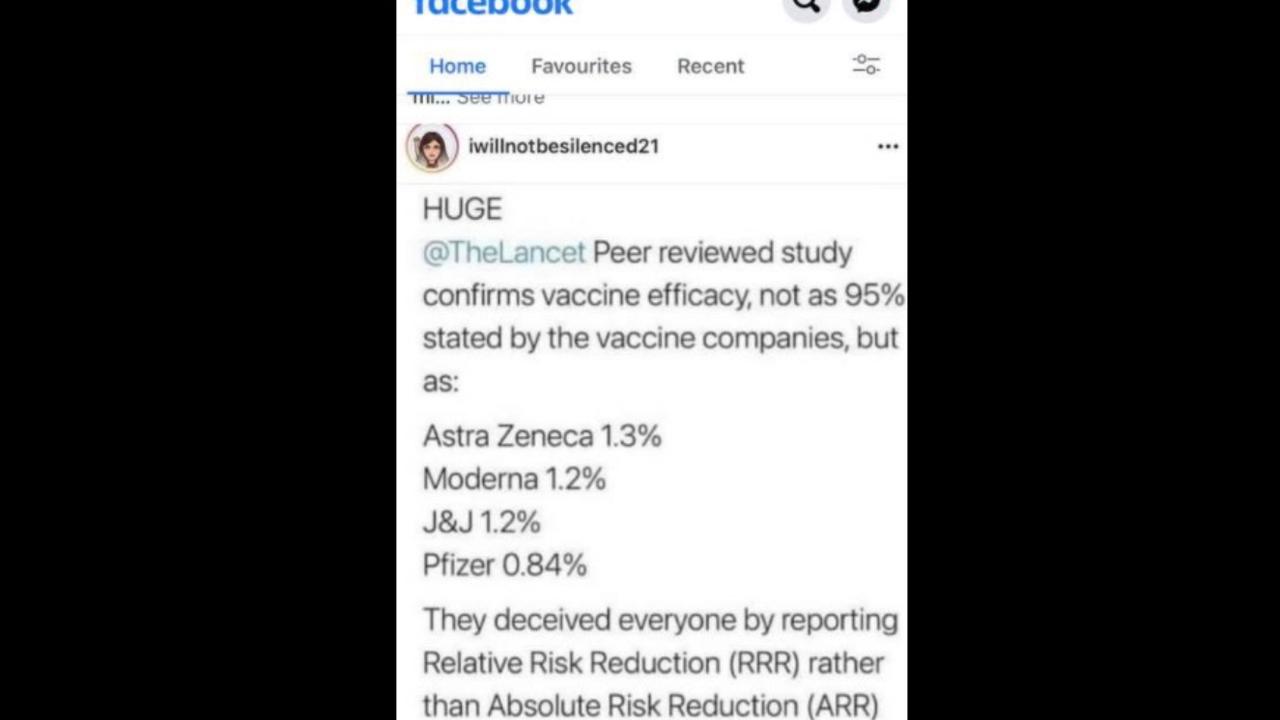
The May 28 Facebook post features a screenshot that says a Lancet study "confirms vaccine efficacy" is not the 95 per cent "stated by the vaccine companies".
It goes on to claim the actual efficacy rates are between 0.84 per cent and 1.3 per cent for various vaccines, adding: "They deceived everyone by reporting Relative Risk Reduction (RRR) rather than Absolute Risk Reduction (ARR)."
The post was from a Facebook account for Australian Jamie McIntyre, who has previously shared misinformation regarding COVID-19 and vaccines. Similar claims have also been shared by social media accounts in Canada and the UK.
The Analysis
Claims that vaccine efficacy rates are much lower than commonly cited figures misinterpret The Lancet article - which is a commentary piece not a peer-reviewed study - that has been used to support the suggestion.
The article does not say that COVID-19 vaccines are ineffective nor that their publicly quoted efficacy rates are wrong, only that multiple measures of efficacy should be used to properly determine the benefits of a vaccine.
The Lancet Microbe article, written by academics in the UK and Luxembourg, argues that absolute risk reduction (ARR) figures should be cited alongside relative risk reduction (RRR) rates when vaccine trial results are outlined in order to avoid reporting bias and to ensure public health decisions around which vaccines to deploy are based on a "full picture" of the data. Vaccine efficacy is commonly reported in only RRR terms following clinical trials.
The figures listed in the Facebook post are the ARR rates included in the article for four vaccines commonly used in Western countries.
However, contrary to the post's suggestion that the ARR rates show vaccines' true efficacy, the different rates do not contradict each other or show that the vaccines are largely ineffective.
Rather, RRR shows the reduction in risk of an outcome based on an intervention - in this case, the reduced chance of contracting COVID-19 after being inoculated against the virus. In comparison, as explained by Meedan Health Desk experts, ARR is simply the difference in infection rates between the intervention group and the placebo group.
Paul Glasziou, the director of the Institute for Evidence-Based Healthcare at Bond University, gave a hypothetical example of the difference between the two measures: Over the next year a patient had a two per cent chance, but by performing a treatment that risk was reduced to one per cent.
"That's a 50 per cent relative reduction (RRR), in other words you're halving the number of people who would get an event out of those who would get it," he told AAP FactCheck.
"But it's an absolute one per cent reduction because you've gone from two per cent to one per cent."
Piero Olliaro, a co-author of The Lancet article and professor of poverty-related infectious diseases at the University of Oxford, told AAP FactCheck in an email the article did not suggest that vaccines did not work.
"It is extremely disappointing to see how information can be twisted and how divisive discussions have become especially on COVID-19 vaccines ...These vaccines are good public health interventions," he said.
Associate professor James Wood, an expert in mathematical modelling and infectious diseases epidemiology at UNSW Sydney, said there are limitations with using ARR to measure a person's risk of getting COVID-19.
"The basic problem with this idea is that it assumes that the absolute risk observed in the trial is a good measure of your risk of getting COVID without the vaccine. It's not - trials are of limited duration (only a few months), and we expect that without a vaccine pretty much everyone will eventually be exposed to COVID," Dr Wood said in an email.
"Using ARR would be highly misleading about eventual risks of contracting COVID-19 in the absence of vaccination, and vastly underestimates the benefits of the vaccines."
As noted in The Lancet article, ARR figures are influenced by background factors such as the infection rate within a given population. Dr Glasziou noted the time frame in which data was collected also affected ARR rates, while RRR figures generally remained steady.
Vaccine efficacy rates shown in clinical trials have since been backed up by data from various international rollouts. A US analysis showed the Pfizer and Moderna vaccines were at least 90 per cent effective in preventing infection in real-world settings, while another set of data from Israel put the Pfizer vaccine's effectiveness at stopping infection at 95 per cent.
Further data, yet to be peer-reviewed, suggests the AstraZeneca vaccine (page 5) offers a similar level of protection from symptomatic illness.
Similar claims have been debunked by other fact-checking organisations here, here and here.
The Verdict
The post misrepresents The Lancet article, which is a commentary piece and not a peer-reviewed study as claimed. The article does not say COVID-19 vaccines are ineffective or that their widely cited efficacy rates are wrong, only that multiple measures should be used to assess vaccines' overall effectiveness.
Pharmaceutical companies have not "deceived" people as to vaccines' effectiveness as the measures referred to in the study represent the same information in two different ways that are not contradictory. Real-world data suggests COVID-19 vaccines are highly effective in reducing the risk of infection or illness.
False – Content that has no basis in fact.
AAP FactCheck is an accredited member of the International Fact-Checking Network. To keep up with our latest fact checks, follow us on Facebook and Twitter.